
Glioblastoma Definitions and Explanations
A glioblastoma (GBM) diagnosis can be overwhelming for patients, caregivers, and families alike. To help you navigate through this complex journey, Gray for Glioblastoma has compiled essential definitions and explanations of key terms related to GBM. This guide will support you by offering clarity on medical terms, treatment options, and potential next steps in your glioblastoma experience. If you are looking for more general glioblastoma resources, including education and medical guidance, support groups, nutrition and wellness, legal planning, clinical trials, and caregiver resources, please visit our General GBM Resource Center.
What is Glioblastoma / GBM / Glioblastoma Multiforme?
All three names refer to the same disease. Glioblastoma multiforme (GBM) is the full name; glioblastoma and GBM are the shorthand versions used interchangeably. It is a grade 4 malignant brain tumor — the highest grade, meaning the fastest-growing and most aggressive classification. It originates in glial cells, which are the support cells of the brain and spinal cord.
What is a Malignant Tumor?
A malignant tumor refers to cancerous growths that can invade nearby tissues and spread to other parts of the body. These tumors grow uncontrollably and are capable of metastasizing—spreading beyond their original location, making them more difficult to treat (Cancer.gov).
Grade 4 / WHO Classification
Cancer grade refers to how abnormal the cancer cells appear under a microscope. Tumors are graded from roman numerals I to IV, with lower-grade tumors (I and II) growing more slowly and being less likely to grow into (invade or infiltrate) nearby tissues. Higher-grade tumors (III and IV), such as glioblastomas, grow rapidly and are more invasive, requiring more intensive treatments. Glioblastomas are always classified as grade 4 brain cancer.
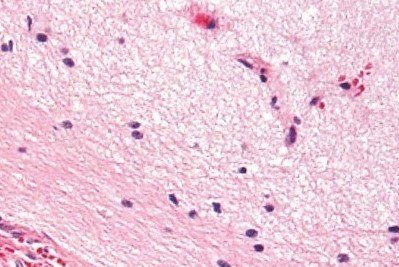
“Normal brain cells”

“Glioblastoma brain cells”
What is MGMT Methylation?
MGMT is a DNA repair gene. When the promoter region of that gene is methylated (essentially switched off), the tumor loses its ability to repair DNA damage caused by chemotherapy. That means chemotherapy — specifically temozolomide — is significantly more effective. MGMT-methylated tumors respond better to treatment and are associated with longer survival. Your pathology report will say methylated or unmethylated.
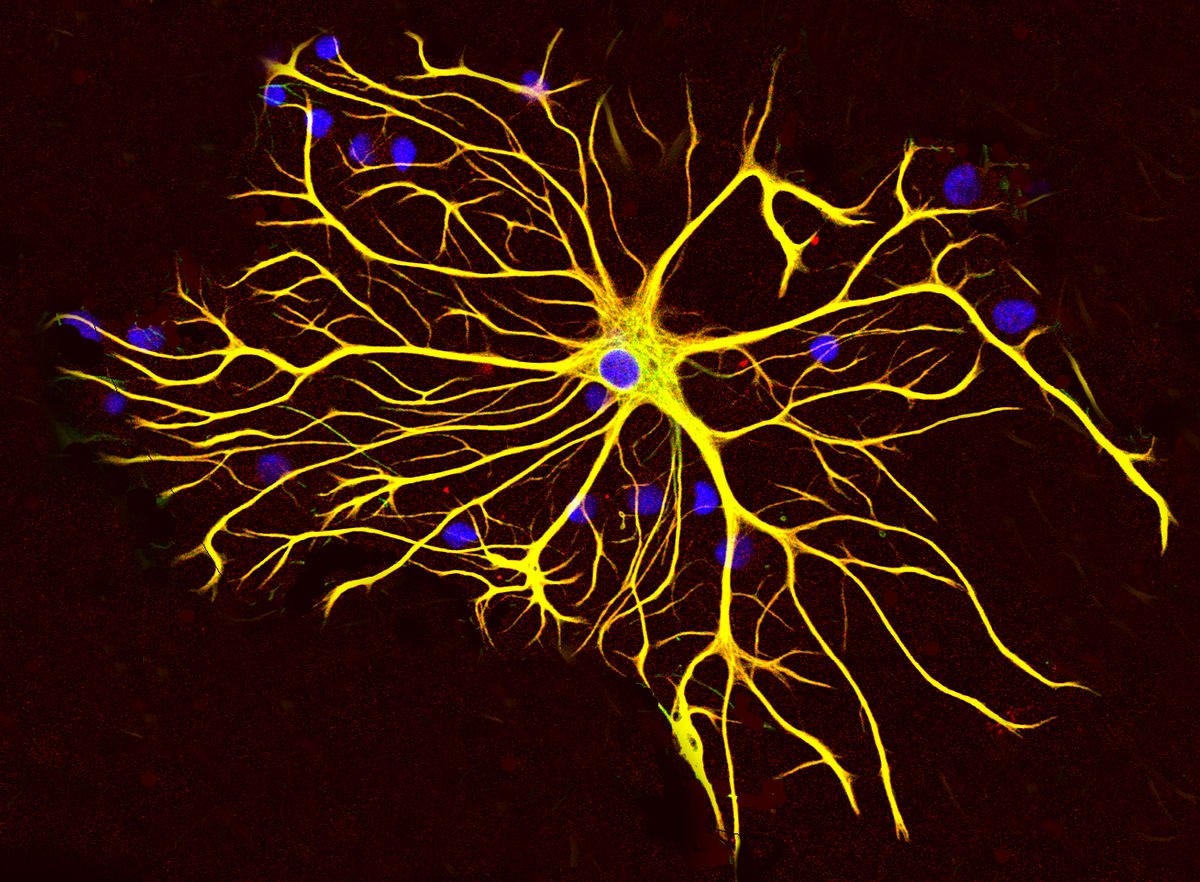
What is an Astrocytoma?
Astrocytomas are tumors that arise from astrocytes—star-shaped glial cells that make up the “glue-like” or supportive tissue of the brain (ABTA).
What is EGFR Amplification?
EGFR stands for epidermal growth factor receptor. In GBM, the EGFR gene is amplified (overactive) in roughly half of cases, which drives tumor growth. It's a marker your oncologist will look at, particularly when assessing clinical trial eligibility. Several targeted therapies aimed at EGFR are currently in trials.
What is a Biopsy?
A biopsy is the removal of a small sample of tumor tissue for analysis. In GBM, this usually happens during surgery — the surgeon removes as much of the tumor as possible and sends the tissue to pathology. In cases where surgery isn't immediately possible, a stereotactic biopsy (a minimally invasive needle biopsy guided by imaging) may be performed first to get a diagnosis before deciding on next steps.
Pathology Report / Molecular Profile
After surgery, the tumor tissue is sent to a pathology lab for analysis. The report that comes back is called a pathology report or molecular profile. It tells your oncology team the specific genetic fingerprint of your tumor — IDH status, MGMT methylation, EGFR status, and other markers. This report shapes every treatment decision that follows. Ask your oncologist to walk through it with you in plain language; it is yours to understand, not just file away.
What is a Craniotomy?
A type of procedure performed on the brain while you are awake and alert. During the procedure, doctors place your head in a fixed position to keep your head still and ensure surgical accuracy. Some of your hair may be clipped to do this. An anesthesiologist will give you some medication to make you sleepy for parts of your awake brain surgery. Your neurosurgeon will apply numbing medications to your scalp to ensure your comfort. During surgery, a team of speech-language pathologist may ask you questions or ask you to identify pictures or words on cards, make movements, count numbers or raise a finger. Your responses help your surgeon identify and avoid damage to the functional areas in your brain (Mayo Clinic). Recovery varies, but most patients are in the hospital for 2–5 days post-surgery, with a longer recovery at home.
What does Recurrence / Recurrent GBM mean?
Recurrence occurs when cancer cells that were previously undetectable or believed to have been completely removed or treated start to grow again. This can happen in the same location where the cancer originally appeared (local recurrence), in nearby tissues (regional recurrence), or in distant parts of the body (distant recurrence).
Glioblastoma is known for its high rate of recurrence due to its aggressive nature and the challenge of completely removing or treating all tumor cells (Mayo Clinic). According to the Central Brain Tumor Registry of the United States Statistical Report, about 90 percent of patients with glioblastoma will experience a recurrence.
What is Pseudoprogression?
Shortly after completing radiation, an MRI may appear to show the tumor growing. This can be pseudoprogression — not actual tumor growth, but an inflammatory response to radiation that looks like tumor activity on a scan. It's more common in patients with MGMT-methylated tumors. Distinguishing true progression from pseudoprogression is genuinely difficult and sometimes requires additional imaging, time, or biopsy. If your first post-treatment MRI looks alarming, ask specifically whether pseudoprogression is being considered.
What is The Blood-Brain Barrier?
A selective permeability barrier between the bloodstream and the central nervous system. It can make delivering treatments to the brain more challenging. The BBB is a selective barrier made up of tightly joined cells lining the blood vessels in the brain. It separates the brain’s blood supply from the brain tissue itself. One of the biggest challenges with this barrier is that it can also prevent many therapeutic drugs from reaching the brain. This makes treating brain conditions, like glioblastoma, more difficult because many chemotherapy drugs and other treatments cannot easily cross the barrier. Scientists are studying ways to bypass or temporarily open the barrier to deliver treatments more effectively.
What are Glial Cells / Glioma?
Glial cells are the support cells of the brain — they surround and protect neurons, help maintain the brain's chemical environment, and assist with immune function. A glioma is any tumor that originates in glial cells. Glioblastoma is the most aggressive type of glioma. Other gliomas include astrocytomas and oligodendrogliomas, which are typically slower-growing.
Maximal Safe Resection
The surgical goal in GBM treatment. It means removing as much tumor as possible without causing new neurological damage — preserving function while maximizing the extent of removal. The amount of tumor removed (called extent of resection, or EOR) is one of the most significant factors in outcomes. Gross total resection (GTR) means the entire visible tumor was removed; subtotal resection (STR) means a portion was left behind due to location or safety concerns.
What is Temozolomide (TMZ / Temodar)?
Temozolomide is the chemotherapy drug at the center of standard GBM treatment. It's taken as an oral pill — not an IV infusion — which is notable. It works by damaging the DNA of cancer cells so they can't replicate. TMZ is given during radiation (daily, at a lower dose) and then for six or more additional cycles after radiation ends (at a higher dose, for five days out of every 28). Its effectiveness is significantly influenced by MGMT methylation status.
What is Radiation?
After surgery, radiation is used to target the tumor site and the surrounding area where microscopic cells are likely present. Standard GBM treatment involves 30 fractions (sessions) of radiation over 6 weeks, Monday through Friday. Each session takes about 15–30 minutes. Radiation is delivered by a machine called a linear accelerator (LINAC). You won't feel anything during sessions. Side effects — fatigue, temporary hair loss in the treated area, skin irritation — build gradually and typically peak in the weeks after treatment ends
What is Dexamethasone?
Dexamethasone is a corticosteroid — a powerful anti-inflammatory drug. It is almost always prescribed immediately after a GBM diagnosis to reduce swelling and inflammation in the brain caused by the tumor and surgery. It works quickly and can provide rapid symptom relief. It is not a cancer treatment itself — it manages the brain's response to the tumor. Side effects of dexamethasone can be significant and confusing if you're not warned about them: increased appetite and weight gain, mood changes (including irritability, anxiety, or emotional swings), difficulty sleeping, elevated blood sugar, and with long-term use, muscle weakness and immune suppression. These are normal responses to the drug, not new symptoms of the disease. The goal is always to taper dexamethasone to the lowest effective dose as quickly as is safe.
Tumor Treating Fields (TTFields / Optune)
Tumor Treating Fields is a therapy that uses low-intensity, alternating electrical fields to disrupt the process by which cancer cells divide. It is delivered through the Optune device — a wearable system consisting of transducer arrays (electrode patches) that adhere to the shaved scalp, connected by wires to a portable battery pack worn in a shoulder bag or backpack. The device needs to be worn for as many hours a day as possible — the recommended minimum is 18 hours. Clinical trial data showed that adding TTFields to standard maintenance chemotherapy extended median survival compared to chemotherapy alone, which is why it became part of standard-of-care guidelines in the US. The practical reality of Optune is significant: you shave your head, apply the arrays every few days, manage skin irritation underneath the patches, and carry the device everywhere. Many patients adapt and find it manageable. Others find it significantly affects quality of life. It is a personal decision that deserves an honest conversation with your oncology team — and with other patients who have been through it.
What is Bevacizumab (Avastin)?
Bevacizumab is a targeted therapy drug that works by cutting off the blood supply to tumors — a process called anti-angiogenesis. It is FDA-approved for recurrent GBM and is often used when the tumor returns after initial treatment. It can reduce tumor-related swelling and may allow patients to taper off dexamethasone. It has not been shown to extend overall survival in newly diagnosed GBM, but it can improve quality of life and is a meaningful tool at recurrence
What is Levetiracetam (Keppra)?
Levetiracetam (Keppra) is the most widely used drug for anti-seizures. It is usually reserved only for patients that have experienced tremors or seizures.
Clinical Trial / Phase I, II, III
A clinical trial is a research study that tests a new treatment — or a new combination of existing treatments — in real patients. For GBM patients, clinical trials are not a last resort — they are often the most important option to pursue, especially at diagnosis and at recurrence. Ask about trial eligibility at every stage of treatment. Trials are the pathway through which new GBM treatments become available. They happen in phases:
Phase I: Tests safety and dosing in a small group. The primary question is: is this tolerable in humans?
Phase II: Tests whether the treatment shows signs of effectiveness in a larger group.
Phase III: Compares the new treatment against current standard of care in a large, randomized group. A successful Phase III trial is the gateway to FDA approval.
Visit our resources page to access clinical trial finders
What is the Tumor Microenvironment (TME)?
The tumor microenvironment is the ecosystem surrounding a tumor — the mix of immune cells, blood vessels, structural proteins, and signaling molecules that the tumor lives within and actively manipulates. GBM is particularly skilled at creating a hostile, immunosuppressive microenvironment that blocks immune cells from reaching it. Many emerging therapies are designed to reshape the TME — making it more vulnerable to immune attack rather than targeting the tumor cells directly.
What is a Personalized / Neoantigen Vaccine?
A cancer vaccine for GBM is not a prevention vaccine — it's a treatment vaccine. It works by training the immune system to recognize and attack the specific proteins (called neoantigens) that are unique to an individual's tumor. Because every GBM tumor has a slightly different molecular fingerprint, the most promising vaccine approaches are personalized — custom-built for each patient using their tumor's genetic data.
What is CAR-T Cell Therapy?
CAR-T (chimeric antigen receptor T-cell) therapy is a form of immunotherapy in which a patient's own T-cells (immune cells) are extracted, genetically engineered in a lab to recognize a specific target on cancer cells, and then infused back into the patient. It has shown dramatic results in certain blood cancers. Early GBM trials have had mixed but increasingly promising results, and it is one of the most actively watched areas of brain cancer research.
What is Immunotherapy?
Immunotherapy refers to treatments that work by stimulating or enabling the body's own immune system to recognize and attack cancer cells. It has transformed outcomes in several cancers — melanoma, lung cancer, and others. In GBM, immunotherapy has been more challenging due to the blood-brain barrier and the tumor's ability to create an immunosuppressive environment that hides it from immune cells. It remains one of the most active areas of GBM research, with checkpoint inhibitors, CAR-T cell therapy, and cancer vaccines all under investigation.
-
When the location of the brain tumor is the Frontal lobe it may cause difficulty with:
Concentrating or focusing attention, speaking, communication skills and language production, controlling emotions and behavior, executive functions such as making decisions, solving problems, planning and organizing, learning and remembering new information, lack of inhibition, social , impulse control and sexual behavior, weakness on the opposite side of the body from the tumor, loss of smell.
-
When the location of the brain tumor is the parietal lobe it may cause difficulty with:
bringing together information from your different senses (touch, vision, hearing, smell, taste) and making sense of it, recognizing faces or objects, co-ordinating movements, spatial awareness (judging distances and hand-eye co-ordination), speaking, understanding words, writing, reading, numbness on the opposite side of the body from the tumor.
-
When the location of the brain tumor is the temporal lobe it may cause:
Difficulty hearing, speaking, identifying and categorizing objects, learning new information, correctly identifying emotions in others, memory loss, seizures or blackouts, sensations of strange smells.
-
When the location of the brain tumor is the occipital lobe it may cause:
difficulty with vision such as identifying objects or colors, loss of vision on one side.
-
When the location of the brain tumor is the cerebellum it may cause:
Difficulty with balance, a loss of co-ordination, difficulty walking or speaking, difficulty using executive functions (making decisions, solving problems, planning and organizing) flickering of the eyes, vomiting, stiff neck, problems with dexterity (skills in using your hands).
-
When the location of the brain tumor is the Brain Stem/Spinal Cord it may cause:
Unsteadiness, difficulty walking, facial weakness, double vision, difficulty speaking and swallowing.
Tumor Location
Depending on where glioblastoma tumors develop in the brain, the symptoms and treatment approaches can vary. Glioblastoma can occur in various regions of the brain, affecting different functions. The main regions affected include…